
TL;DR:
- Effective pharmaceutical research requires meticulous preparation, strict compliance, and operational pragmatism across all stages from discovery to post-market surveillance.
- Balancing scientific rigor with operational realities and risk-based management strategies enhances efficiency, reduces costs, and ensures regulatory success.
Pharmaceutical research doesn’t forgive shortcuts. Whether you’re advancing a small molecule candidate or a complex biologic, knowing how to conduct pharmaceutical research with methodological rigor is what separates successful drug programs from costly failures. The obstacles are real: regulatory hurdles, data integrity demands, participant safety requirements, and clinical trial design complexity all create pressure points where programs stall or collapse. This guide walks you through every critical stage, from early target identification through post-market surveillance, so your organization can execute with confidence and stay on the right side of the FDA every step of the way.
Table of Contents
- Understanding the pharmaceutical research process
- Preparation essentials: setting up for successful pharmaceutical research
- Executing clinical trials effectively: phases and best practices
- Verifying and ensuring compliance for reliable pharmaceutical research outcomes
- The overlooked essentials in pharmaceutical research: insight from experienced practitioners
- Partner with Veridata Insights for compliant, efficient pharmaceutical research
- Frequently asked questions
Key Takeaways
| Point | Details |
|---|---|
| Comprehensive preparation | Thorough preclinical studies and well-prepared IND applications are critical to successful pharmaceutical research initiation. |
| Adherence to GCP | Following Good Clinical Practice guidelines ensures participant safety and data reliability throughout clinical trials. |
| Risk-based quality management | Prioritizing critical quality factors improves trial efficiency while maintaining high standards and compliance. |
| Regulatory readiness | Maintaining clean, well-documented data and processes minimizes FDA audit risks and clinical trial holds. |
| Pragmatic operational insights | Early focus on scalable manufacturing and pragmatic record keeping streamlines drug development beyond theoretical compliance. |
Understanding the pharmaceutical research process
To conduct pharmaceutical research effectively, you need to see the full pipeline before you zoom in on any single phase. The drug development journey is long, expensive, and highly regulated, and underestimating that scope upfront leads to poor planning downstream.
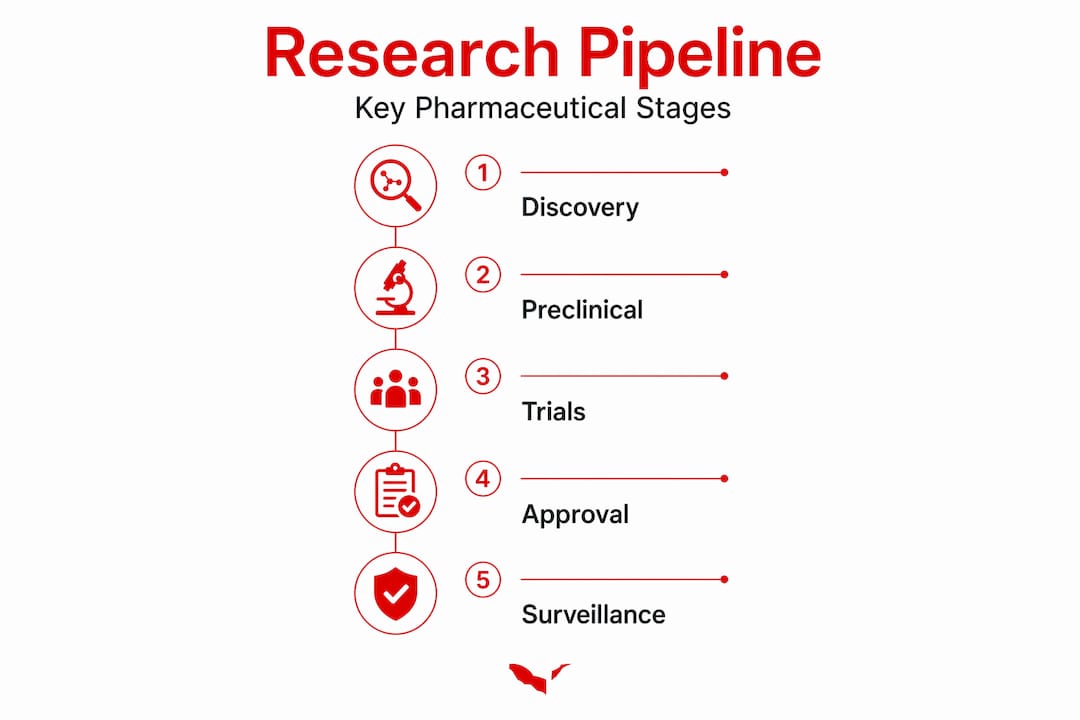
The drug development process includes discovery, preclinical research, clinical trial phases I through IV, regulatory submission, and post-market surveillance. Each stage has distinct goals and non-negotiable standards. The average program spans 12 to 15 years and costs over a billion dollars before a single prescription is written.
Here’s what each major phase is designed to accomplish:
- Discovery: Identify and validate a biological target linked to the disease. Generate lead compounds with potential therapeutic effect.
- Preclinical research: Test candidates in laboratory models and at least two animal species. Assess safety, toxicology, and pharmacokinetics before any human exposure.
- Phase I clinical trials: Establish safety and dosing in a small group of healthy volunteers or patients.
- Phase II clinical trials: Evaluate preliminary efficacy and refine dosing in a targeted patient population.
- Phase III clinical trials: Confirm efficacy and safety at scale across thousands of subjects in multiple sites.
- Regulatory approval: Submit a New Drug Application (NDA) or Biologics License Application (BLA) to the FDA for review.
- Phase IV and post-market surveillance: Monitor the drug in the real-world population for long-term safety signals and rare adverse events.
Success at each stage depends on maintaining pharmaceutical research compliance from day one. Organizations that treat compliance as an afterthought routinely pay for it in clinical holds and resubmission delays.
Preparation essentials: setting up for successful pharmaceutical research
With a clear understanding of the pharmaceutical research process, meticulous preparation for each stage is what keeps execution on track. Most programs that stumble do so because of gaps in the preparatory groundwork, not the science itself.
Target identification and validation is where it all starts. Your therapeutic target must be scientifically validated through both biological evidence and disease relevance. Rushing this step leads to expensive late-stage failures.
Preclinical research typically requires two to three years of testing across at least two animal models under Good Laboratory Practice (GLP) standards. GLP is a formal quality system that governs how preclinical safety studies are planned, performed, recorded, and reported. This isn’t a formality. It’s the foundation your IND application rests on.

The Investigational New Drug (IND) application is your gateway to human trials. An IND application must contain preclinical safety data, manufacturing documentation, and clinical protocols, with the FDA completing its review within 30 calendar days. If you submit an incomplete or disorganized IND, you’re looking at a clinical hold before you’ve enrolled a single participant.
Key preparation steps at a glance:
- Validate your therapeutic target with peer-reviewed evidence
- Design GLP-compliant preclinical studies across at least two animal models
- Document Chemistry, Manufacturing, and Controls (CMC) thoroughly
- Assemble clinical protocols with clearly defined endpoints and participant criteria
- Submit your IND and begin the 30-day FDA review clock
- Build quality assurance documentation practices from the start, not after your first audit
| Preparation stage | Primary requirement | Common mistake |
|---|---|---|
| Target validation | Scientific evidence of disease relevance | Skipping competitive target analysis |
| Preclinical studies | Two animal models, GLP compliance | Single-species testing |
| IND assembly | CMC, preclinical data, clinical protocols | Incomplete manufacturing documentation |
| FDA submission | 30-day review, clinical hold risk | Submitting before data package is clean |
| QA documentation | SOPs and audit trails from day one | Retrofitting documentation post-trial |
Investing early in data integrity and compliance infrastructure pays dividends when the FDA auditor walks through the door. The cost of remediation is always higher than the cost of prevention.
Pro Tip: Before submitting your IND, conduct an internal mock review using FDA’s own IND review criteria. Assign team members to evaluate each section as if they were the agency. You’ll catch gaps your internal team has become blind to.
Executing clinical trials effectively: phases and best practices
After preparing your IND and preclinical foundation, executing clinical trials systematically with clear phase objectives and rigorous data practices is what produces results you can actually submit to regulators.
Each phase has a defined purpose. Blurring those boundaries or trying to answer too many questions in a single trial is one of the most common and costly mistakes in pharmaceutical study design.
Step-by-step trial execution by phase:
- Phase I: Enroll 20 to 100 healthy volunteers to assess safety, pharmacokinetics, and appropriate dosing over several months. The goal is not efficacy. It is safety and tolerability.
- Phase II: Move to your target patient population. Refine dosing, identify preliminary efficacy signals, and document adverse events in a controlled setting.
- Phase III: Enroll 1,000 to 3,000 subjects across multiple sites over six or more months to confirm efficacy and safety at scale. This is your pivotal data for regulatory submission.
Best practices for conducting clinical trials:
- Define inclusion and exclusion criteria with specificity before recruitment opens. Vague criteria create protocol deviations and data quality problems.
- Use placebo or active controls where ethical and scientifically appropriate to strengthen your efficacy evidence.
- Implement Good Clinical Practice (GCP) standards per ICH E6(R2/R3), which govern risk-based monitoring, data integrity, and human subject protection.
- Build real-time adverse event monitoring into your trial management systems. Waiting for a safety review meeting to catch a signal is too slow.
- Train site staff on protocol adherence before enrollment starts, not during the trial.
| Trial phase | Enrollment size | Primary objective | Duration |
|---|---|---|---|
| Phase I | 20 to 100 | Safety, pharmacokinetics, dosing | Months |
| Phase II | 100 to 300 | Preliminary efficacy, dose refinement | Months to 2 years |
| Phase III | 1,000 to 3,000 | Efficacy and safety confirmation | 1 to 4 years |
Good risk-based clinical trial management means concentrating monitoring resources where the risk to data quality and participant safety is highest, not spreading attention uniformly across every site and data point. That approach saves time without cutting corners.
Ethical clinical trial design also means honest informed consent, ongoing participant monitoring, and a Data Safety Monitoring Board (DSMB) empowered to halt a trial if safety signals emerge. No efficacy outcome justifies participant harm.
Pro Tip: When researching drug interactions during Phase II and III, use a pre-specified interaction analysis plan locked before unblinding. Post-hoc interaction analyses are viewed skeptically by regulators and rightly so.
Verifying and ensuring compliance for reliable pharmaceutical research outcomes
Once clinical trials are executed, thorough verification and compliance procedures are what convert raw trial data into regulatory-accepted results. This stage is where programs either cement their credibility or unravel it.
Quality assurance and standard operating procedures (SOPs) at every trial stage, including site monitoring and data cleanup, are non-negotiable before any FDA audit. An audit-ready organization doesn’t scramble when the FDA calls. It opens its documentation and waits.
Compliance verification essentials:
- Conduct regular internal audits against your SOPs before an external inspection
- Close all protocol deviations with documented corrective and preventive actions (CAPAs)
- Validate all data entry and electronic systems against 21 CFR Part 11 requirements
- Ensure all adverse event reporting timelines are met and documented
- Maintain complete investigator site files and sponsor files with audit trails intact
“Sponsors must implement risk-based quality management focusing on critical-to-quality factors per ICH E6(R3) 2025.” — ICH E6(R3) implementation guidance
The ICH E6(R3) framework is the current gold standard for clinical quality management. It asks you to identify what is truly critical to participant safety and data credibility, then focus your resources there. Not everything in a trial carries equal risk. Treating it all the same wastes effort and misses what matters.
FDA IND review timelines are 30 days, and approximately 10 to 15% of submissions receive clinical holds. A clinical hold is not a death sentence, but it delays your program and signals documentation or safety gaps the FDA isn’t comfortable proceeding past.
Post-market surveillance rounds out the compliance picture. After approval, your obligation to patient safety doesn’t end. Phase IV trials and ongoing pharmacovigilance programs generate the long-term safety data regulators and prescribers rely on. Organizations that treat post-market work as bureaucratic overhead consistently face preventable safety crises.
Pro Tip: Don’t wait for the FDA to identify data anomalies. Use statistical process control methods to monitor your own data streams in real time. Catching a data quality issue internally is far less disruptive than receiving a query during an inspection.
Proactively avoiding pharmaceutical research pitfalls and investing in fraud prevention practices through the full research lifecycle keeps your data defensible and your program moving.
The overlooked essentials in pharmaceutical research: insight from experienced practitioners
Here’s something most compliance guides won’t tell you: the parts of pharmaceutical research that sink programs are rarely the parts everyone talks about. They’re the unglamorous, operational details that get deprioritized until they become emergencies.
Take manufacturing scale-up. Significant gaps exist between lab-scale synthetic routes and scalable GMP (Good Manufacturing Practice) processes. The SELECT framework, which covers Safety, Environment, Legality, Economics, Control, and Throughput, gives teams a practical way to evaluate manufacturing decisions early. Most organizations don’t apply it until Phase II, by which point they’ve already locked in process choices that are expensive to reverse.
The instinct to perfect your synthetic route before scaling up sounds responsible. In practice, it often means pouring resources into a lab process that will never survive manufacturing conditions. Practical optimization for GMP from the start beats theoretical elegance every time.
Electronic records are another area where we see unnecessary complexity. Certified copies of electronic records are sufficient for retention purposes, as long as context, content, structure, and metadata are preserved. This means organizations don’t need to maintain every original file in multiple formats across multiple systems, as long as the certified copy is complete and traceable. Streamlining this process meaningfully reduces compliance overhead without creating regulatory risk.
Our broader experience in cost-effective pharmaceutical research confirms what the data shows: organizations that adopt pragmatic, risk-based approaches earlier in the research lifecycle move faster and with fewer surprises. The ones that treat every process as equally critical end up paralyzed by their own rigor. That’s not compliance. That’s anxiety wearing compliance’s clothes.
The most effective pharmaceutical study design balances scientific ambition with operational reality. Custom research approaches built around your specific program and regulatory context will outperform a templated methodology borrowed from a program with different constraints every single time.
Partner with Veridata Insights for compliant, efficient pharmaceutical research
With these methodologies in hand, the next step is putting them to work with partners who understand the full complexity of pharmaceutical research, not just pieces of it. Veridata Insights brings deep expertise in compliance-driven research design aligned with ICH E6(R3) risk-based quality management standards, along with data quality solutions that keep your trial data defensible from collection through audit. Whether you need support with electronic data strategy, audit readiness, or participant recruitment for hard-to-reach healthcare populations, we work with you 7 days a week, 365 days a year, with no project minimums and no one-size-fits-all approach. Contact Veridata Insights today to build a research strategy that holds up under scrutiny.
Frequently asked questions
What are the main stages of pharmaceutical research?
Pharmaceutical research includes discovery, preclinical testing, clinical trials across Phases I through III, regulatory approval, and post-market surveillance to confirm ongoing safety and efficacy.
How long does preclinical research typically take?
Preclinical research typically takes two to three years and involves testing in at least two animal models under Good Laboratory Practice standards before an IND can be submitted to the FDA.
What is the FDA review timeline for an IND application?
The FDA reviews IND applications within 30 calendar days; the IND automatically becomes effective on day 30 unless the agency issues a clinical hold due to safety or documentation concerns.
What are the key compliance standards during clinical trials?
Clinical trials must comply with Good Clinical Practice per ICH E6, which emphasizes participant protection, risk-based monitoring, and data integrity throughout trial execution and reporting.
How can pharmaceutical companies ensure data integrity and readiness for FDA audits?
By implementing SOPs and quality assurance at every trial stage, including proactive data cleanup, documented corrective actions, and real-time adverse event monitoring, companies can maintain data integrity and face FDA audits without scrambling.












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}