
TL;DR:
- A pharmaceutical survey methodology workflow is a structured process to ensure the collection of valid, reliable data for drug development and market analysis. Strict adherence to design, sampling, execution, and analysis standards is essential for regulatory approval and accurate results.
A pharmaceutical survey methodology workflow is the structured process researchers use to collect valid, reliable data for drug development and market analysis. In the pharma industry, this process is also called clinical survey methodology or research survey design, and it covers everything from defining endpoints to delivering regulatory-ready reports. Getting it right is not optional. Poorly designed surveys produce data that notified bodies reject, market analyses that mislead, and development decisions that cost millions to reverse. This guide walks you through every stage of a rigorous survey workflow, from objective setting through final analysis.
What are the essential components of a pharmaceutical survey methodology workflow?
A complete workflow for pharmaceutical research has four core stages: design, sampling, execution, and analysis. Each stage depends on the one before it. Skipping or rushing any stage introduces bias that compounds downstream.

Stage 1: Objective setting and endpoint definition
Every survey starts with a clearly stated research objective and defined endpoints. Primary endpoints drive sample size calculations and statistical tests. Secondary endpoints capture supporting data, such as safety signals or prescribing behavior patterns. Without this clarity upfront, your questionnaire will collect noise alongside signal.
Stage 2: Questionnaire construction
Questions must map directly to clinical data fields. PMCF surveys, for example, must generate Level 4 clinical evidence by mapping each question to extractable patient chart fields and embedding adverse event detection within every case. General opinion polling does not meet notified body standards. Every question earns its place by serving a defined endpoint.
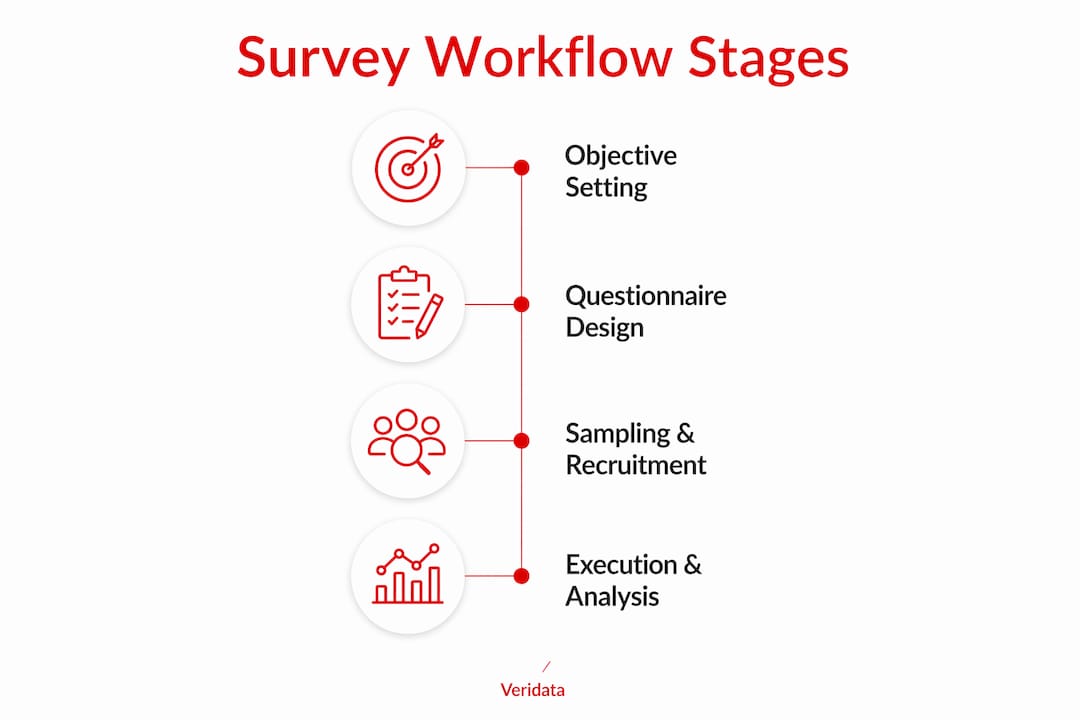
Stage 3: Sampling and recruitment
Sampling strategy determines who answers your survey and whether the results generalize. Pharma surveys use both probability and non-probability methods depending on the research phase. Inclusion and exclusion criteria must be documented before recruitment begins, not adjusted after data collection starts.
Stage 4: Execution and analysis
Survey administration, monitoring, and statistical analysis form the final stage. This is where quality controls either protect your data or fail it.
Key workflow components to track across all four stages:
- Research objective: Stated in one sentence with measurable outcomes
- Primary and secondary endpoints: Defined before questionnaire construction begins
- Adverse event capture: Embedded within each survey case for regulated studies
- Sampling documentation: Written justification for method selection and sample size
- Statistical plan: Significance levels, power calculations, and drop-out adjustments confirmed before launch
Pro Tip: Write your statistical analysis plan before you finalize your questionnaire. If a question cannot feed your analysis plan, cut it.
How do you design pharmaceutically rigorous survey questionnaires?
Questionnaire design is where most pharma surveys fail. Researchers either ask too many questions, use ambiguous language, or borrow question formats from consumer research that have no clinical validity. The pharmaceutical research checklist approach works: every item on your questionnaire must justify its presence against a clinical or regulatory criterion.
Here is a proven construction sequence for pharma questionnaires:
- Map endpoints to question types. Closed-ended, structured questions produce extractable data. Open-ended questions generate qualitative texture but require coding before analysis. Use closed-ended formats for primary endpoints and reserve open-ended items for exploratory secondary questions.
- Apply the KAP framework. Knowledge, Attitude, and Practice (KAP) surveys structure questions to capture clinical constructs without overloading respondents. KAP is particularly effective for physician surveys measuring prescribing behavior and treatment decision drivers.
- Use Discrete Choice Experiments for benefit-risk questions. DCE methodology provides a structured framework covering attribute identification, experimental design, questionnaire construction, and statistical analysis to quantify patient benefit-risk preferences. A fractional factorial design reduces scenario complexity from over 1,000 possible profiles to a manageable choice set, often using SAS macros to generate the design matrix.
- Sequence questions strategically. Clinical outcome questions come first. Satisfaction questions appear only if needed and never before primary endpoint items. Respondents give their best attention early. Do not waste it on low-priority items.
- Control survey length. Fatigue degrades data quality in the final third of long surveys. Pilot test with five to ten respondents from your target population and measure completion time. Aim for under 20 minutes for physician surveys and under 15 minutes for patient surveys.
Pro Tip: Add two to three reliability check items, such as reverse-worded versions of key questions, to flag respondents who are rushing or not reading carefully. Remove their data before analysis.
Visual aids improve response accuracy for complex clinical scenarios. A diagram showing a drug administration device, for example, reduces misinterpretation of questions about handling and usability. Use them selectively where ambiguity is a real risk.
Which sampling methods optimize pharmaceutical survey results?
Sampling method selection is a strategic decision across a drug’s lifecycle, balancing statistical rigor with practical access to niche populations. The wrong method produces data that looks valid but cannot support regulatory or commercial conclusions.
| Sampling method | Best use case | Key limitation |
|---|---|---|
| Simple random sampling | Large, accessible populations | Impractical for rare disease groups |
| Stratified random sampling | Subgroup comparisons across physician specialties | Requires known population proportions |
| Purposive sampling | Expert panels, key opinion leader research | Results do not generalize statistically |
| Snowball sampling | Hard-to-reach patient communities | High risk of selection bias |
| Quota sampling | Market research with defined segment targets | Non-random, limits inferential statistics |
Probability sampling suits confirmatory validation studies where statistical generalizability is required. Non-probability methods work for early-stage exploratory research where speed and access to niche groups matter more than representativeness.
Key factors that drive sampling decisions in pharma:
- Population rarity: Rare disease populations require non-probability methods because probability sampling is simply not feasible at scale
- Regulatory expectations: Confirmatory studies submitted to notified bodies require documented probability sampling with power calculations
- Budget and timeline: Non-probability methods are faster and cheaper but carry higher bias risk
- Drop-out adjustment: A statistically justified sample size accounts for a 10–20% drop-out or non-evaluable rate, using a significance level of 0.025 (one-sided) or 0.05 (two-sided). That buffer is not optional in regulated studies. It is the difference between a study that survives regulatory review and one that gets sent back for more data.
Document your sampling rationale in writing before recruitment begins. Regulators and notified bodies expect to see the justification, not just the result. For more detail on effective sampling strategies, the method you choose should always connect back to your research objective.
What are best practices for executing and analyzing pharmaceutical surveys?
Survey execution is where well-designed studies either hold together or fall apart. Administration platform, monitoring frequency, and response rate management all affect data integrity.
Administration platform selection depends on your respondent population. Online platforms broaden reach and reduce data entry errors through built-in validation rules. Paper surveys remain necessary for some clinical settings where respondents lack digital access or where regulatory requirements specify paper-based documentation. Hybrid approaches combine both, but they require harmonized data entry protocols to prevent format inconsistencies.
Response rate management is an active process, not a passive hope. Low response rates and variable engagement require proactive monitoring and respondent encouragement strategies to preserve data quality. Reminder protocols at 7, 14, and 21 days after initial contact are standard practice. Personalized reminders outperform generic ones. Incentive structures must comply with applicable regulations and institutional review board requirements.
Real-time monitoring catches problems before they become fatal. Track completion rates, drop-off points, and response time per question. A sudden spike in time spent on one question signals a comprehension problem. A high drop-off rate at a specific item means that item needs revision or removal.
Statistical analysis must follow the pre-specified analysis plan. Primary endpoint analyses use the significance levels defined during design. Secondary analyses are clearly labeled as exploratory. Pharma market research techniques include quantitative analytics for treatment preferences and prescribing trends, complemented by qualitative coding for open-ended responses. Never run unplanned analyses and present them as confirmatory findings.
Reporting for regulatory scrutiny requires a structured report that documents the research objective, methodology, sampling rationale, response rates, data cleaning steps, statistical outputs, and limitations. Notified bodies and ethics committees expect to see the full chain of evidence, not just the headline findings.
Key takeaways
A pharmaceutical survey methodology workflow produces defensible, regulatory-ready data only when design, sampling, execution, and analysis each follow documented, pre-specified standards.
| Point | Details |
|---|---|
| Define endpoints first | Set primary and secondary endpoints before writing a single survey question. |
| Map questions to clinical fields | Every question must connect to an extractable data field or a defined endpoint. |
| Justify your sample size | Account for a 10–20% drop-out rate and document your significance level in writing. |
| Monitor execution in real time | Track completion rates and drop-off points to catch problems before they corrupt your data. |
| Follow a pre-specified analysis plan | Run only the analyses you defined before data collection to maintain scientific credibility. |
Where most pharma survey workflows actually break down
I have reviewed a lot of pharma survey projects, and the failure point is almost never the statistics. It is the gap between what researchers intend to measure and what their questionnaire actually captures. A team will spend weeks on sample size calculations and then write questions that a consumer research firm would reject for being too vague. That disconnect is where data quality dies.
The rise of Discrete Choice Experiments is genuinely exciting for benefit-risk research. DCE gives you a structured way to quantify what patients actually trade off when choosing between treatments, not what they say they prefer in a direct question. But DCE is not a plug-and-play solution. The fractional factorial design requires real statistical expertise, and I have seen teams use it without fully understanding the attribute levels they selected. The output looks rigorous. The inputs were not.
Digital survey platforms have made execution faster and cheaper. That is mostly good news. The risk is that speed encourages skipping the pilot test. A 20-minute pilot with five physicians from your target specialty will catch more problems than a week of internal review. Do not skip it because the platform makes launch feel easy.
The other thing I keep seeing: researchers treat the sampling documentation as a formality. They write it after the fact to match what they actually did. Regulators are not fooled. Write your sampling rationale before recruitment starts. It forces clearer thinking and it protects you when a notified body asks why you made the choices you made.
For anyone conducting pharmaceutical research, the most underrated skill is knowing when to simplify. More questions do not produce better data. A focused 12-item survey with clean clinical mapping will outperform a 40-item survey with mixed question quality every time.
— Daniel
How Veridata Insights supports your pharma survey workflow
Veridata Insights works with pharmaceutical researchers and healthcare professionals who need survey methodology done right, from the first consultation through final reporting. Whether you need PMCF survey design that meets notified body standards, DCE questionnaire construction, or full-service data collection and analysis, the team at Veridata Insights handles it. There are no project minimums, and support is available seven days a week. If your research requires hard-to-reach physician or patient populations, Veridata Insights specializes in exactly that kind of recruitment. Contact Veridata Insights to discuss your next pharmaceutical survey project and get a workflow built around your specific research objectives.
FAQ
What is a pharmaceutical survey methodology workflow?
A pharmaceutical survey methodology workflow is the end-to-end process of designing, sampling, executing, and analyzing surveys to collect valid clinical or market data. It covers everything from endpoint definition to regulatory-ready reporting.
How do PMCF surveys differ from standard market research surveys?
PMCF surveys must generate Level 4 clinical evidence by mapping questions to patient chart fields and embedding adverse event detection within each case. Standard market research surveys do not carry these regulatory requirements.
What sample size should a pharma survey use?
Sample size depends on your primary endpoint, significance level, and expected drop-out rate. A statistically justified calculation typically adds a 10–20% buffer for drop-outs, using a significance level of 0.025 or 0.05.
When should you use a Discrete Choice Experiment in pharma research?
Use a DCE when you need to quantify patient benefit-risk preferences across multiple treatment attributes. DCE is particularly effective when direct preference questions would oversimplify complex trade-offs between efficacy, safety, and convenience.
What causes low response rates in pharmaceutical surveys?
Low response rates result from survey length, poor timing, lack of personalized outreach, and unclear respondent incentives. Proactive reminder protocols at regular intervals and concise, clinically relevant questionnaires are the most effective countermeasures.












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}